
| Not so much artistic, but mostly photos of wildflowers and wild fauna uploaded to iNaturalist. | View robertkamper’s observations » |
Mother’s Day

My mother, who died at the age of 79, over 30 years ago. May she rest in peace. This is a photo of her in her 30s, taken in the 1940s.
The title of this blog refers to living well with a misdiagnosis. My mother was one of those “mistakes” that doctors make, and then bury. She had complained of stomach pain early in the year, and her general practitioner physician pooh-poohed it as remnants of stomach flu or some such thing, instead of ruling out the worst case scenario and following a logical path to an accurate diagnosis. By the time she was actually diagnosed and real doctors were able to take a look, the pancreatic cancer was too advanced to treat, and passed away a few months later in great pain that even heavy doses of morphine were unable to mitigate. At her funeral gathering we sang her favorite church hymn: I Sing A Song Of The Saints of God
Living with a misdiagnosis… (continued)
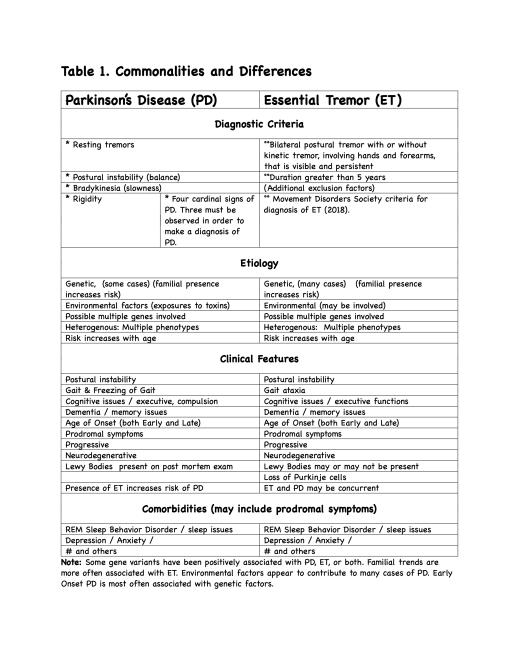
In two previous posts of part of this unpublished article we provided the results in the form of a table, which listed diagnostic criteria and some common features and symptoms of Essential Tremors (ET) and Parkinson’s Disease (PD), and the basic Abstract section.
Today, we will look at the Discussion section, beginning with Quality of Life (QOL) impacts, and the Conclusions, listed as a half dozen null hypotheses.
Discussion:
The subject reports the following impacts on QOL:
· Failure to correctly identify, diagnose, and treat underlying conditions in a timely manner resulted in career termination prior to 60 years.
· Human interactions, both person to person and in public speaking, were affected by presence of hand tremors as well as vocal tremors.
· Open disclosure of diagnosis affected interpersonal relations of all kinds – some for better, some not.
· Interactions and side effects of various medications and treatments. (Risks from DBS and chronic administration levodopa are of concern (Vyavahare, S, et al., (2025)), including:
· Mood disorders,
· Balance, gait, and fall risk issues,
· Excessive daytime somnolence,
· Weight gain and loss,
· Libido and sexual functioning,
· Functions of organs such as kidneys and liver.
· General anhedonia and dysphoria.
· Financial impacts due to costs of medical insurance, medical services, medications and treatments, and diminished earning ability
The subject asks the following questions regarding QOL:
· How does one measure the loss of over a decade of one’s life due to a misdiagnosis?
· How does one calculate the loss of earnings and savings spent to pay for DBS surgery and follow up treatments?
· How does one calculate the hours spent on purchasing, tracking, and dispensing medications and supplements over a decade?
· Which of the numerous falls over the years (including a fractured femur) may have been avoided if he had not been misdiagnosed, mistreated, and over medicated?
The subject admits his situation could have been worse: misdiagnosis or missed diagnosis did not result in death.
The subject also admits that following the misdiagnosis of PD after seeking treatment for ET, he read as much research as possible, and noted the multiple prodromal and other risk factors in his history. He embraced the diagnosis of PD, exhibiting his own confirmation bias, and failed to fully explore the research on ET and ET concurrent with PD. Failure to seek or to recommend a second opinion regarding diagnosis and treatment with DBS is a responsibility shared by both patient and physician.
Factors affecting Early, Timely, Accurate, and Effective Diagnoses and Treatments
The stigma of being “sick” in a society which values the lower two of Moses Maimonides’s four ways in which man seeks perfection, can have negative effects. (The four types of perfection are (1.) wealth, titles, and power over others, (2.) physique and personal appearance, (3.) ethical virtue (social behavior to benefit others), and (4.) development of rational virtue (logic, science, and metaphysics) (Maimonides, The Guide of the Perplexed, (1952) translated by Rabin, C., abridged version by Guttman, J,)
The lowest of these is the “perfection of wealth.” In a system in which health care is not considered a basic human right, and ethical virtue does not assist in the attainment of amassing of wealth, some people are drawn to careers related to medicine as a means to attain perfection of wealth.
Consider the following data:
· In 2024 alone, pharmaceutical and health products companies reported over 16 million transfers or payments totaling $13.18 Billion to health care providers (https://openpaymentsdata.cms.gov/about accessed 20 September, 2025).
· Over $388 Million was spent to lobby on behalf of these companies during the year 2024, with over $226 Million reported so far in 2025 (https://www.opensecrets.org/industries/lobbying?cycle=2024&ind=H04 accessed 21 September, 2025).
· Recorded contributions to political campaigns from the industry in 2023-2024 were over $86 Million (https://www.opensecrets.org/industries/totals?cycle=2024&ind=H04 accessed 21 September 2025).
Note: All of the above funds were legally spent and reported. How much of the $13.8 Billion total was in the form of discounts or free services to patients is not known. Unknown whether any of the money spent lobbying and donating to political entities reduced the cost of healthcare for patients with Parkinson’s Disease, or any individual patient’s medical cost burden.
In addition to the seductive influence of wealth on diagnosis and treatment options (such as DBS and new versions of carbidopa-levodopa medications), physicians may also delegate the actual provision of services to others under their supervision.
Some neurologists may, in the face of what has been dubbed a “Parkinson’s Pandemic” (Dorsey,R. & Okun, M. (2025)), expand their practice beyond their actual areas of expertise, whether motivated by the attainment of wealth or a genuine attempt to provide services in an area in which there are too few MDSs to meet the needs of the population.
The bottom line IS the bottom line. The health system is not focused on the needs of patients, but on the profits required to provide investors with the best possible return on investment. Reflecting on the QOL issues, it may be the case that an investment in providing services to patients would provide a greater return on investment in the long run than in considering people to be as fungible as funds.
Conclusions:
Null Hypotheses and expected conclusions are presented based on reviewed research articles and abstracts, primarily from PubMed Central (https://pmc.ncbi.nlm.nih.gov/).
Null hypothesis 1:
· PD and ET are distinct conditions and easily diagnosed by General Practitioners using the current diagnostic criteria.
Conclusion:
· Expect Rejection of Null Hypothesis (ERNH). Initial diagnoses of ET, PD, and other movement disorders are well below 100% in initial clinical presentations. (Joutsa et al., 2014, Adler et al. 2014, Khan et al. 2024)
Null hypothesis 2:
· PD and ET do not share any common features or symptoms.
Conclusion:
· (ERNH). Multiple common features and symptoms (See Table 1).
Null hypothesis 3:
· PD and/or ET are wholly due to genetic factors.
Conclusion:
· (ERNH). ET and PD cases are heterogenous in etiology. (See Table 1).
Null hypothesis 4:
· PD and/or ET are simply due to natural aging processes.
Conclusion:
· (ERNH). Age increases risk, but is not determining factor (See Table 1).
Null hypothesis 5:
· Interactions with medications, environmental factors, and genetics do not need to be considered when diagnosing or treating ET or PD.
Conclusion:
· (ERNH). Criteria for ET specifically notes certain drug interactions as a factor for exclusion. (Bhatia et al., 2018). (However, MDS criteria do not include genetics (presence in family members) as a criterion for diagnosis of ET.) Recommendation: MDS should consider adding family history and DNA analyses to diagnostic criteria for ET and PD.
Null hypothesis 6:
· History of ET diagnosis is unrelated to progression of PD symptoms following PD diagnosis.
Conclusion:
· (ERNH). ET history in patients with PD is associated with a benign prognosis with slower motor and non-motor symptoms progression.” (Ou, R.,et al., 2020; Cutrona et al., 2025).
Recommendations and implications for practice and research:
The low accuracy of initial diagnosis for PD should be noted when conducting research, reviews and metareviews. Although several initiatives to develop algorithms to predict risks for developing PD have been created, these mathematical models are vulnerable to missing or undocumented data, which reduces the accuracy of these tools.
Further longitudinal investigation to include subjects with
1. Existing diagnosis of ET to identify those who
1.1. Later develop PD (ET + PD),
1.2. Do not later develop PD (ET only), and
1.3. Subjects who do not have a diagnosis of either ET or PD (control group)
2. Investigate subjects with current family histories of
2.1. ET,
2.2. ET+PD, and
2.3. absence of either ET or PD.
3. Continue studies into relationship between tremors and disease progression.
4. Include DNA analysis and broaden genes included in correlation, as has been initiated.
Implications for practice:
Clinician education and patient education are in need of greater effort and attention in order to improve early identification and treatments.
Clinicians and Physicians
· Clinicians need to be conscious of and defend against confirmation bias which could lead to misdiagnosis and missed diagnoses, impacting the patient’s Quality Of Life or mortality, including inviting patients to seek
· Physicians and clinicians need to exercise caution to avoid iatrogenic symptoms, toxic medicine interactions, and other complications.
· Physicians need to put patient needs at the center of their practice.
· Or, in other words, FIRST, DO NO HARM (Consider hanging as a reminder poster in all physicians’ offices)?
• Patients (and caregivers) need to
- Seek second opinions before major operations such as DBS,
- Educate self regarding conditions and treatments,
- Check for side effects of treatments
- Take responsibility to ensure all members of the medical care team are advised and kept up to date on treatments
More research into shared and concurrent symptoms of related movement disorders is needed, given the difficulty of diagnosis and concurrence of many prodromal and post onset symptoms
End of this post.
References may be posted later. Maybe not.
A brief excursion…
Took a side trip with the Master Gardeners class group to the Oklahoma Tulip Farm in Harrah, OK, the other day. Tulips were blooming in various stages and colors, and I took a few photos:
The first is a view at the farm outbuilding on the adjacent property, posterized and framed between the barbed wire fence.

The next few are of tulips, of course:




Some days, you need to take a break from the “brief excursions” of what passes for reality, and remind oneself what reality is like in the real world of this tiny outpost in the vast emptiness of space, the cosmos, and appreciate the quiet times.
###
Living well with a misdiagnosis: abstract
This is a continuation of the last post, which presented the RESULTS section of this article, as Table 1. This is the Abstract.
Living Well With (a Misdiagnosis of) Parkinson’s Disease
ABSTRACT
GOAL:
To review research related to
· Difficulty of diagnosis among and between movement disorders,
· Factors leading to misdiagnosis,
and
· Quality of Life issues experienced
BACKGROUND:
Single Subject Case Study of a 76 year old male. First reported Essential Tremor (ET) symptoms dating to teenage years. ET became disabling after five decades. ET refractory to treatment by a neurologist. Deep Brain Stimulation (DBS) chosen by subject as a last resort. Prior to DBS implants, a diagnosis of Parkinson’s Disease (PD) was made, due to rigidity observed A DATScan performed seven years after diagnosis reportedly showed abnormal dopamine transport..
Thirteen years after PD diagnosis, subject relocated and was referred to a Movement Disorders Specialist (MDS). On examination, no PD symptoms were observed. MDS began differential diagnosis based on symptoms of tremors, fatigue, and gait abnormality.
At this time, it appears that the subject’s initial presentation and diagnosis of ET (in 2010) was accurate. The later diagnosis of PD was vulnerable to confirmation bias, apparently the neurologist treating for ET had identified gait abnormality as rigidity, and failed to rule out other possible causes for arm swing asymmetry (Navarro-López et al., 2022). Heterogeneity of tremors (Fekete & Li, 2013) apparently was not investigated. Interestingly, in one of the case studies reported by Fekete & Li, a patient had been diagnosed as PD by a different neurologist, and was later determined to have ET without concurrent PD. It is not lost on this author that the references noted are later than the misdiagnosis (in December 2011). “If I knew then what I know now…”
METHODS:
Review of research articles available on PubMed Center relevant to
· Diagnostic criteria,
· Prodromal symptoms,
· Accuracy of diagnoses,
· Differentiating symptoms between ET, ET and PD, and PD.
In addition, discussion includes observable and subjective data regarding subject’s
Quality of life (QOL), including but not limited to:
· Side effects of medications,
· Dosages of medications,
· costs of medications
· Impacts of side effects, dosage, and costs for unnecessary medical interventions on other aspects of individual and social quality of life.
· Factors related to diagnosis and misdiagnosis.
Next: Quality of Life and Factors Affecting Misdiagnosis
###
My Personal Journey with Medical Misdiagnosis
Or, What I did last Summer
We remember, fondly or not, typical school essay topics:
- What I did last summer
- How my family celebrates the winter holidays
- What America means to me
- My favorite (TV, movie, book, song, musical group)
- Things my parents tell me not to tell other people
- The greatest American President
I once wrote an essay about a relative. I actually took the question seriously, instead of offering the usual platitudes. I pondered on a negative experience: the untimely death of a child. This loss could have been prevented with more timely reliance on medical providers. Of course, this happened well before penicillin became widely available for treatment of appendicitis or peritonitis. As a parent, I promptly responded when my child complained of abdominal pain. She was treated for appendicitis and survived.
This past year, my summer was also related to a missed diagnosis. Fortunately, no one died, although I had been treated for the wrong condition for over a dozen years. It has been said that physicians bury their mistakes. Not this time. Instead, the differential diagnosis and removal of medications triggered research into the differentiation between Essential Tremors and Parkinson’s Disease. Another side effect was rewording this blog’s subtitle, replacing PD with Movement Disorder.
I submitted an abstract to the World Parkinson’s Conference. It will be held in May of 2026. Unfortunately, the abstract didn’t make the cut. Perhaps the abstract failed to include enough information, perhaps it didn’t have a positive enough bias in its presentation. Whatever. The research found misdiagnosis of movement disorders is not uncommon. Therefore I’ve decided to share it through this medium. Some people will find value in it.
Below is a table from the article. In future posts, parts of the article will be shared, including the discussion, conclusions, and references by category.
Snow and ice will suffice
It’s been nearly a third of a year since I last posted on this site. Advancing years, physical therapy, adjusting to changes in medications and dealing with sleep disorders has kept this off my list of priorities.
So, instead of getting into a list of what has or hasn’t happened during the hiatus, today we’ll look at today and yesterday, as Oklahoma and much of the nation is experiencing a winter storm.

This angular composition is the result opening the kitchen door. Interesting (to me, anyway) are the layers of the snow drift against the door, somewhat analogous to the rings of a tree. As can be seen, we had at least an initial overnight snowfall, followed by three snowfalls of lesser duration or intensity.

Raising our sights up a little, tracks of an unobserved critter are seen between a tree tentatively identified as Cedar Elm (Ulmus crassifolia). The critter leaving tracks is probably either an Eastern Fox Squirrel (Sciurus niger) or Eastern Gray Squirrel (Sciurus carolinensis). Because the Fox squirrel is adaptable to a variety of habitats and is listed as the most common species of squirrel in Oklahoma, it seems these are likely the tracks of a Fox squirrel. The Gray is smaller and prefers densely wooded forests, according to the OSU Gray and Fox Squirrels fact sheet.

Finally, a look out the front door and the texture of snow with a slight line of demarcation between the sidewalk and the minimal porch, providing an illusion of the overcast clouds in the sky.
And if you didn’t catch the allusion in the title…
Clematis and Milkweeds, welcome to the family…
One of my favorite “flowers” is the female Clematis drummondii which is most noticeable in the late summer as the achenes turn into cascades of clouds that give it one of its common names, Old Man’s Beard. The actual flower is shown in the first photo following, the achenes in the other two:



Another favorite plant is Matelea reticulata, commonly known as Pearl Milkweed Vine, due to the “pearl” in the middle of its flower. It, too, is native to Central Texas, where I no longer reside, having “pulled up roots” to move a bit further to the North.



I was pleasantly surprised to find, recently, a different Clematis, native to Central Oklahoma. Clematis terniflora, or Autumn Clematis, as it’s commonly known, is smaller than its Texas cousin, but still provides striking clouds of white flowers and achenes along the roadsides and in ditches. In this case, the flowers provide the show, and the achenes are less showy than those of C. drummondii, as seen in the third photo following:



Cynanchum laeve, common name Honey Milkweed Vine, has been observed in several locations around here, notably near the airport and a few miles away. As suggested by the common name, the flowers give off a strong, sweet smell attractive to humans and pollinators alike.


While they’re not the same species one has become accustomed to, the “new” species are familiar enough to provide a sense of a welcoming environment.
###
Spring Photos of Three Oklahoma Tree Species
A few photos from Bethel Acres in Central Oklahoma during. the Spring of 2025.
The first focuses on the long needles and early cones before they’ve matured. According to an Audubon Society Field Guide published in 1980, this species is native only to the Southeastern tip of Oklahoma. The Wildflower Center’s Native Plants database page, updated in 2022, repeats this information. The location where this photo was taken, of a tree distributed without human intervention, shows the effects of global warming in the extension of its range northward. (Assuming the species is identified correctly.)

Next is what appears to be a Post Oak, with a three lobed leaf shape. The leaves are about 5 to 8 inches long, but shape and size are highly variable.


Blackjack Oak (Quercus marilandica)
Finally, here’s a Blackjack Oak, which has much larger catkins than the Post Oak. The two different species are known to hybridize easily. Perhaps we will post some photos in the future. Observed what appeared to be a Post and a Blackjack oak, growing next to each other, and each showing leaves resembling the “template” form for both pf the species. The typical Blackjack Oak leaf has a “duck foot” shape, almost triangular, without any deep indents. The Post Oak, on the other hand, has a “head” lobe with two deep indents above and below what look like “arms,” tapering a little into the form of a (vaguely) human body.
But that’s a task for another day.
Me and My PD – Misdiagnosis and Confirmation Bias
Non-Artificial Intelligence Summary: The author reveals that he was misdiagnosed with Parkinson’s Disease (PD) over 13 years ago, after initially seeking treatment for Essential Tremors (ET). The article concludes with a link to an open access article on Six Myths and Misconceptions about Essential Tremor.
_________________________
Over the summer of 2025, I’ve been undergoing review of my movement disorders, with a reduction in medications as well as no clinical observation of Parkinson’s Disease (PD) symptoms.
Some thirteen or so years ago, after a neurologist or nurse practitioner observed some slight rigidity, providing enough symptoms to make a clinical diagnosis, an old high school girlfriend called to express some concern and to wish me the best. Apparently, she was under the misconception that PD was equivalent to a slow death. Glad to say she must be mighty disappointed after all these years.
I had essential tremors (ET) from my teen years, in addition to several other prodromal conditions or symptoms relating to PD. In 2010 the ET had become somewhat disabling, and after many months of unsuccessful treatment for ET, I opted for Deep Brain Stimulation (DBS), which apparently had a great success rate with ET. However, in order to rule out PD, several months of tests were undergone, with the eventual three of four of the cardinal signs being observed. DBS was scheduled less than two months later. Seven years later, due to a lack of progressive neurological deterioration, a DAT Scan was ordered, with an interpretation that I apparently did have some form of parkinsonism. Apparently, the original diagnosis of PD was premature and made under the influence of confirmation bias. Or, to paraphrase Paul Simon, a person sees what they want to see and disregards the possibility of other underlying causes for a barely detectable symptom.
Finally, after moving to a different state and establishing care with a Movement Disorder Specialist, who conducted their own evaluation on and off PD medications, the original problem (ET) which brought me to a neurologist in 2010, was confirmed. The process of titrating off medications continues.
Naturally, I have been delving into the National Institutes of Health open access in order to learn more about what has been called “familial tremors” and “benign tremors” in the past.
One thing I have learned is the diagnosis of ET and PD can be difficult, due to many overlapping symptoms or conditions, they are linked genetically for some ET cases, and much of the material on PD doesn’t even investigate whether the two conditions are concurrent.
So another reason for me to go on living: educate and advocate for people who may or may not have a diagnosis appropriate to their condition.
We’ll start here, with a recent article on Six Myths and Misconceptions about Essential Tremor.
