In two previous posts of part of this unpublished article we provided the results in the form of a table, which listed diagnostic criteria and some common features and symptoms of Essential Tremors (ET) and Parkinson’s Disease (PD), and the basic Abstract section.
Today, we will look at the Discussion section, beginning with Quality of Life (QOL) impacts, and the Conclusions, listed as a half dozen null hypotheses.
Discussion:
The subject reports the following impacts on QOL:
· Failure to correctly identify, diagnose, and treat underlying conditions in a timely manner resulted in career termination prior to 60 years.
· Human interactions, both person to person and in public speaking, were affected by presence of hand tremors as well as vocal tremors.
· Open disclosure of diagnosis affected interpersonal relations of all kinds – some for better, some not.
· Interactions and side effects of various medications and treatments. (Risks from DBS and chronic administration levodopa are of concern (Vyavahare, S, et al., (2025)), including:
· Mood disorders,
· Balance, gait, and fall risk issues,
· Excessive daytime somnolence,
· Weight gain and loss,
· Libido and sexual functioning,
· Functions of organs such as kidneys and liver.
· General anhedonia and dysphoria.
· Financial impacts due to costs of medical insurance, medical services, medications and treatments, and diminished earning ability
The subject asks the following questions regarding QOL:
· How does one measure the loss of over a decade of one’s life due to a misdiagnosis?
· How does one calculate the loss of earnings and savings spent to pay for DBS surgery and follow up treatments?
· How does one calculate the hours spent on purchasing, tracking, and dispensing medications and supplements over a decade?
· Which of the numerous falls over the years (including a fractured femur) may have been avoided if he had not been misdiagnosed, mistreated, and over medicated?
The subject admits his situation could have been worse: misdiagnosis or missed diagnosis did not result in death.
The subject also admits that following the misdiagnosis of PD after seeking treatment for ET, he read as much research as possible, and noted the multiple prodromal and other risk factors in his history. He embraced the diagnosis of PD, exhibiting his own confirmation bias, and failed to fully explore the research on ET and ET concurrent with PD. Failure to seek or to recommend a second opinion regarding diagnosis and treatment with DBS is a responsibility shared by both patient and physician.
Factors affecting Early, Timely, Accurate, and Effective Diagnoses and Treatments
The stigma of being “sick” in a society which values the lower two of Moses Maimonides’s four ways in which man seeks perfection, can have negative effects. (The four types of perfection are (1.) wealth, titles, and power over others, (2.) physique and personal appearance, (3.) ethical virtue (social behavior to benefit others), and (4.) development of rational virtue (logic, science, and metaphysics) (Maimonides, The Guide of the Perplexed, (1952) translated by Rabin, C., abridged version by Guttman, J,)
The lowest of these is the “perfection of wealth.” In a system in which health care is not considered a basic human right, and ethical virtue does not assist in the attainment of amassing of wealth, some people are drawn to careers related to medicine as a means to attain perfection of wealth.
Consider the following data:
· In 2024 alone, pharmaceutical and health products companies reported over 16 million transfers or payments totaling $13.18 Billion to health care providers (https://openpaymentsdata.cms.gov/about accessed 20 September, 2025).
· Over $388 Million was spent to lobby on behalf of these companies during the year 2024, with over $226 Million reported so far in 2025 (https://www.opensecrets.org/industries/lobbying?cycle=2024&ind=H04 accessed 21 September, 2025).
· Recorded contributions to political campaigns from the industry in 2023-2024 were over $86 Million (https://www.opensecrets.org/industries/totals?cycle=2024&ind=H04 accessed 21 September 2025).
Note: All of the above funds were legally spent and reported. How much of the $13.8 Billion total was in the form of discounts or free services to patients is not known. Unknown whether any of the money spent lobbying and donating to political entities reduced the cost of healthcare for patients with Parkinson’s Disease, or any individual patient’s medical cost burden.
In addition to the seductive influence of wealth on diagnosis and treatment options (such as DBS and new versions of carbidopa-levodopa medications), physicians may also delegate the actual provision of services to others under their supervision.
Some neurologists may, in the face of what has been dubbed a “Parkinson’s Pandemic” (Dorsey,R. & Okun, M. (2025)), expand their practice beyond their actual areas of expertise, whether motivated by the attainment of wealth or a genuine attempt to provide services in an area in which there are too few MDSs to meet the needs of the population.
The bottom line IS the bottom line. The health system is not focused on the needs of patients, but on the profits required to provide investors with the best possible return on investment. Reflecting on the QOL issues, it may be the case that an investment in providing services to patients would provide a greater return on investment in the long run than in considering people to be as fungible as funds.
Conclusions:
Null Hypotheses and expected conclusions are presented based on reviewed research articles and abstracts, primarily from PubMed Central (https://pmc.ncbi.nlm.nih.gov/).
Null hypothesis 1:
· PD and ET are distinct conditions and easily diagnosed by General Practitioners using the current diagnostic criteria.
Conclusion:
· Expect Rejection of Null Hypothesis (ERNH). Initial diagnoses of ET, PD, and other movement disorders are well below 100% in initial clinical presentations. (Joutsa et al., 2014, Adler et al. 2014, Khan et al. 2024)
Null hypothesis 2:
· PD and ET do not share any common features or symptoms.
Conclusion:
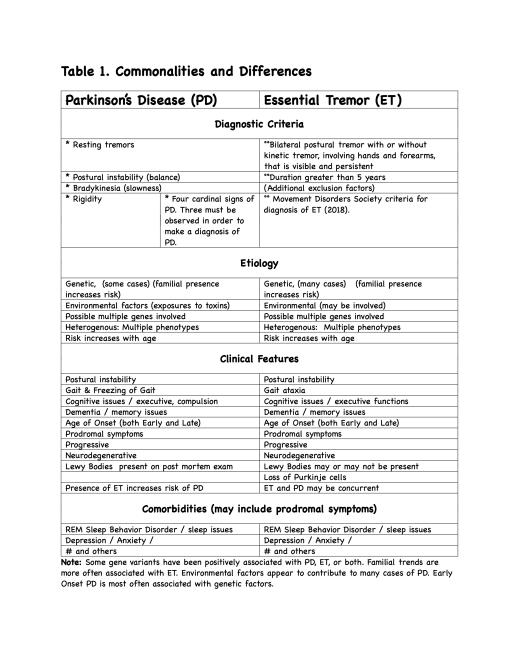
· (ERNH). Multiple common features and symptoms (See Table 1).
Null hypothesis 3:
· PD and/or ET are wholly due to genetic factors.
Conclusion:
· (ERNH). ET and PD cases are heterogenous in etiology. (See Table 1).
Null hypothesis 4:
· PD and/or ET are simply due to natural aging processes.
Conclusion:
· (ERNH). Age increases risk, but is not determining factor (See Table 1).
Null hypothesis 5:
· Interactions with medications, environmental factors, and genetics do not need to be considered when diagnosing or treating ET or PD.
Conclusion:
· (ERNH). Criteria for ET specifically notes certain drug interactions as a factor for exclusion. (Bhatia et al., 2018). (However, MDS criteria do not include genetics (presence in family members) as a criterion for diagnosis of ET.) Recommendation: MDS should consider adding family history and DNA analyses to diagnostic criteria for ET and PD.
Null hypothesis 6:
· History of ET diagnosis is unrelated to progression of PD symptoms following PD diagnosis.
Conclusion:
· (ERNH). ET history in patients with PD is associated with a benign prognosis with slower motor and non-motor symptoms progression.” (Ou, R.,et al., 2020; Cutrona et al., 2025).
Recommendations and implications for practice and research:
The low accuracy of initial diagnosis for PD should be noted when conducting research, reviews and metareviews. Although several initiatives to develop algorithms to predict risks for developing PD have been created, these mathematical models are vulnerable to missing or undocumented data, which reduces the accuracy of these tools.
Further longitudinal investigation to include subjects with
1. Existing diagnosis of ET to identify those who
1.1. Later develop PD (ET + PD),
1.2. Do not later develop PD (ET only), and
1.3. Subjects who do not have a diagnosis of either ET or PD (control group)
2. Investigate subjects with current family histories of
2.1. ET,
2.2. ET+PD, and
2.3. absence of either ET or PD.
3. Continue studies into relationship between tremors and disease progression.
4. Include DNA analysis and broaden genes included in correlation, as has been initiated.
Implications for practice:
Clinician education and patient education are in need of greater effort and attention in order to improve early identification and treatments.
Clinicians and Physicians
· Clinicians need to be conscious of and defend against confirmation bias which could lead to misdiagnosis and missed diagnoses, impacting the patient’s Quality Of Life or mortality, including inviting patients to seek
· Physicians and clinicians need to exercise caution to avoid iatrogenic symptoms, toxic medicine interactions, and other complications.
· Physicians need to put patient needs at the center of their practice.
· Or, in other words, FIRST, DO NO HARM (Consider hanging as a reminder poster in all physicians’ offices)?
• Patients (and caregivers) need to
- Seek second opinions before major operations such as DBS,
- Educate self regarding conditions and treatments,
- Check for side effects of treatments
- Take responsibility to ensure all members of the medical care team are advised and kept up to date on treatments
More research into shared and concurrent symptoms of related movement disorders is needed, given the difficulty of diagnosis and concurrence of many prodromal and post onset symptoms
End of this post.
References may be posted later. Maybe not.