My first draft of this got lost in the computer (Thanks, all you coders who think you know how to create intuitive, ease to use interfaces). So here’s another attempt to get stuff from one location to another. We’ll see how it it goes…
A while back I posted a Powerpoint presentation on research on music, dance, and singing, which cited a review in the Movement Disorders Society (2018, I believe), in which the conclusion was that exercise did not affect Parkinson’s Disease (PD) symptoms. Since then, there have been many more studies on the effects of different modalities of exercise. In this first article, a meta review of publications, found that exercise is good for you if have PD.
The purpose of the review was to compare and rank the types of exercise that improve PD symptoms by quantifying information from randomised controlled trials. Out of 10,474 citations, 250 studies were included involving 13,011 participants. The results (drumroll, please):
Power training (PT) had the best benefits for motor symptoms
Body weight support treadmill training showed the best improvement in balance, gait velocity and walking distance
Robotic assisted gait training had the most benefits for freezing of gait
Dance showed the best benefits for depression
Only Yoga significantly reduced anxiety symptom compared with controls
Only resistance training significantly enhanced sleep quality and cognition
Physical Therapy showed the best results for muscle strength
Five types of therapy showed improvement in concerns about falling versus control groups.
If interested, the full free text is available at the linked citation above. Other reviews have shown different results. Best recommendation is to find a variety of exercises that you enjoy, and do them as often as you can. But don’t try so hard that you wind up hurting yourself.
The second meta review alluded to in the title has to do with sleep disorders.
Fifty-three longitudinal studies of sleep in PD were identified, which included:
Excessive daytime sleepiness,
Insomnia,
Obstructive sleep apnea,
Rapid eye movement sleep behavior disorder (RBD),
Restless legs syndrome, and
Shift work disorder were studied in addition to other studies that had focused on either multiple sleep disorders or broadly on sleep disorders as a whole.
RBD is now considered an established prodromal feature of PD, but other sleep disorders do not clearly increase risk of subsequent PD.
I’ll throw in one last citation. Not just because it plays on the title to one of Bob Dylan’s songs, but also because it is one of many nutritional supplements prescribed to aid in cleaning out neural cell debris in (where else?) Bob’s Brain:
I’m not sure why the line numbers were included in the PDF, my guess is that it is/was pre-publication. At any rate, it just adds to the body of evidence that rhythm and movement helps get rid of the blues.
Music can help people make more positive evaluations of acute exercise as an affective and
113 ergogenic stimulant. A recent meta-analysis of 139 studies revealed that listening to music during
114 acute bouts of exercise and sport activities increases positive affective valence (g = 0.48, CI [0.39,
115 0.56]), reduces ratings of perceived exertion (RPE; g = 0.22, CI [0.14, 0.30]), enhances physical 116 performance (g = 0.31, CI [0.25, 0.36]), and improves oxygen consumption (VO2max; g = 0.15, CI
117 [0.02, 0.27]) compared with activities without music (Terry et al., 2020). These findings support the
118 notion that music helps physical activity to be more joyous, less arduous, and more energetic and
119 efficient, arguably motivating the exerciser to join additional bouts. It is noteworthy that the
120 beneficial effects of music on affect and RPE were not moderated by physical activity intensity in the
121 meta-analysis (Terry et al., 2020), which indicates that music provides psychological benefitsacross
122 the full range of intensities.
Here’s a few studies that came up in my news feed from PubMed Central (PMC) or elsewhere for articles recently published on the topics in which I’m interested – namely, prodromal symptoms related to PD, the relationship of REM sleep disorder and depression to PD, and, of course, the use of singing and dance therapies as complementary approaches to dealing with the symptoms of PD.
The prevalence and duration of non-motor symptoms (NMS) in prodromal Parkinson’s disease (PD) has not been extensively studied. The aim of this study was to determine the prevalence and duration of prodromal NMS (pNMS) in a cohort of patients with recently diagnosed PD.
…subtracted the duration of the presence of each individual NMS reported from the duration of the earliest motor symptom. NMS whose duration preceded the duration of motor symptoms were considered a pNMS. Individual pNMS were then grouped into relevant pNMS clusters based on the NMSQuest domains. Motor subtypes were defined as tremor dominant, postural instability gait difficulty (PIGD) and indeterminate type according to the Movement Disorder Society Unified Parkinson’s Disease Rating Scale revision.
Results: Prodromal NMS were experienced by 90.3% of patients with PD. … males reporting more sexual dysfunction, forgetfulness and dream re-enactment, whereas females reported more unexplained weight change and anxiety. There was a significant association between any prodromalgastrointestinal symptoms and urinary symptoms and the PIGD phenotype.[n.b.: phenotype includes inherent traits or characteristics that are observable]. [Emphases added].
Citation: Durcan R, Wiblin L, Lawson RA, Khoo TK, Yarnall AJ, Duncan GW, Brooks DJ, Pavese N, Burn DJ; ICICLE-PD Study Group. Prevalence and duration of non-motor symptoms in prodromal Parkinson’s disease. Eur J Neurol. 2019 Jul;26(7):979-985. doi: 10.1111/ene.13919. Epub 2019 Mar 1. PMID: 30706593; PMCID: PMC6563450.
Purpose: To explore the effect of sleep disorders, including the probable rapid eye movement (REM) sleep behavior disorder (pRBD) and the daytime sleepiness, on depressive symptoms in patients with early and prodromal PD.
5-year follow-up study showed that sleep disorders, including pRBD and daytime sleepiness, were associated with the increased depressive-related score in individuals with early and prodromal PD.
Conclusion: … Sleep disorders, including pRBD and daytime sleepiness, are associated with depression at baseline and longitudinally, … partially mediated by the autonomic dysfunction in early and prodromal PD, … implication that sleep management is of great value for disease surveillance.
Citation: Ma J, Dou K, Liu R, Liao Y, Yuan Z, Xie A. Associations of Sleep Disorders With Depressive Symptoms in Early and Prodromal Parkinson’s Disease. Front Aging Neurosci. 2022 Jun 10;14:898149. doi: 10.3389/fnagi.2022.898149. PMID: 35754965; PMCID: PMC9226450.
Abstract Background Previous reports suggest that group therapeutic singing (GTS) may have a positive effect on motor symptoms in persons with Parkinson’s disease (PD).
Objective To determine the effect of a single session of GTS on clinical motor symptoms.
Methods Clinical motor symptom assessment was completed immediately before and after 1 hour of GTS in 18 participants.
Results A significant decrease in average scores for gait and posture and tremor, but not speech and facial expression or bradykinesia was revealed.
Conclusion These results support the notion that GTS is a beneficial adjuvant therapy for persons with PD that warrants further research.
Citation: Stegemoller E, Forsyth E, Patel B, et al. Group therapeutic singing improves clinical motor scores in persons with Parkinson’s disease BMJ Neurology Open 2022;4:e000286. doi: 10.1136/bmjno-2022-000286
What research has found its way into the email inbox recently?
Although singing is a nearly universal human behavior, many adults consider themselves poor singers and avoid singing based on self-assessment of pitch matching accuracy during singing (here referred to as singing accuracy), in contrast to the uninhibited singing exhibited by children. In this article, I report results that shed light on how singing accuracy changes across the lifespan, using data from a large online sample, including participants ranging from 6 to 99 years old. Results suggest that singing accuracy improves dramatically from childhood to young adulthood, unperturbed by voice changes during adolescence, and remain at a similarly high level for the remainder of life, exhibiting no strong tendency toward age-related decline. Vocal or instrumental musical training has significant positive effects on singing accuracy, particularly in childhood, though there was no evidence for gender differences. Finally, pitch discrimination varied with age similarly to singing accuracy, in support of views that singing accuracy reflects sensorimotor learning. Taken together, these results are consistent with the view that singing accuracy is a learned motor skill that benefits from engagement and can remain a fruitful endeavor into old age. (emphasis added).
Basically, this says that if you learned how sing accurately when you were young, you can probably sing well into your later years. And, since singing is a learned motor skill, one might assume that it can be learned even as one gets older.
Relevance to folks with Parkinson’s Disease (PD)?
Vocal strength exercises, such as those provided by Power for Parkinson’s as free YouTube video classes, can help with specific Parkinson’s related symptoms:
Many people with PD speak quietly and in one tone; they don’t convey much emotion. Sometimes speech soundsbreathy or hoarse. People with Parkinson’s might slur words, mumble or trail off at the end of a sentence.Most people talk slowly, but some speak rapidly, even stuttering or stammering.
Parkinson’s motor symptoms, such as decreased facial expression, slowness and stooped posture, may add to speech problems. These can send incorrect non-verbal cues or impact the ability to show emotion. Source: https://www.michaeljfox.org/news/speech-swallowing-problems accessed June 20, 2022 (emphasis added).
Since our vocal cords are muscles, and singing is a learned motor skill, we can strengthen those muscles and push against the progressive, degenerative symptoms of PD through exercises that:
remind us to breathe deeply to sustain vocal volume,
improve our posture in order to enable deep breathing,
exercise the muscles of the face and mouth
to enable crisp diction instead of slurring and mumbling, and that
support emotional expression through inflection and singing.
And “Everybody Knows” that if exercise is fun, one is more likely to continue doing it.
Full disclosure: The author has attended Power for Parkinson’s ® vocal exercise classes since their inception in 2016, and co-founded a participant organized singing group (with the late Jeff Berke) in 2015. Therefore, he might be (definitely is) biased in favor of this modality of treatment for vocal and speech related symptoms of PD.
And from the abstract and significance statement of the original (non-open access) article:
Physical exercise improves motor performance in individuals with Parkinson’s disease and elevates mood in those with depression. Although underlying factors have not been identified, clues arise from previous studies showing a link between cognitive benefits of exercise and increases in brain-derived neurotrophic factor (BDNF). (emphasis added).
and:
Exercise has been shown to improve movement and cognition in humans and rodents. Here, we report that voluntary exercise over 30 days leads to an increase in evoked dopamine (DA) release throughout the striatum, and an increase in BDNF in the dorsal (motor) striatum. The increase in DA release appears to require BDNF, indicated by the absence of DA release enhancement with running in BDNF+/- mice. Activation of BDNF receptors using a pharmacological agonist was also shown to boost DA release. Together these data support a necessary and sufficient role for BDNF in exercise-enhanced DA release, and provide mechanistic insight into the reported benefits of exercise in individuals with dopamine-linked neuropsychiatric disorders, including Parkinson’s disease and depression. (emphasis added).
The citation:
Voluntary exercise boosts striatal dopamine release: evidence for the necessary and sufficient role of BDNF, Guendalina Bastioli, Jennifer C. Arnold, Maria Mancini, Adam C. Mar, Begoña Gamallo-Lana, Khalil Saadipour, Moses V. Chao, Margaret E. Rice,Journal of Neuroscience 16 May 2022, JN-RM-2273-21; DOI: 10.1523/JNEUROSCI.2273-21.2022
So that covers why exercise is good for all. But what about what is good for the one?
… there is growing recognition that PD is not a single entity but instead reflects multiple diseases, in which different combinations of environmental, genetic and potential comorbid factors interact to direct individual disease trajectories… The clear consequence of there being distinct diseases that collectively form PD, is that there is no single biomarker or treatment for PD development or progression. We propose that diagnosis should shift away from the clinical definitions, towards biologically defined diseases that collectively form PD, to enable informative patient stratification. N-of-one type, clinical designs offer an unbiased, and agnostic approach to re-defining PD in terms of a group of many individual diseases. . (emphasis added).
The citation links to PubMed where you can download the full article, should you be so inclined. The next citation also links to an open access free article.
In this article, Riggare reports on self tracking done in 2012 (as a Person with Parkinson’s), and the offer the possibility that self-tracking of symptoms and medications can help to inform the physician’s decisions over the course of treatment. In other words, one should be a self-advocate as a patient and work with your physician to achieve the best combination of treatments to address Parkinson’s and its comorbidities. (At least that’s my takeaway from the article. Others might differ).
Another look at PD aims to categorize it into various sub-types:
This article is a “desk review”of other studies, using specific criteria to either include/exclude each study in the results. Their conclusion:
Conclusion: Subtyping studies undertaken to date have significant methodologic shortcomings and most have questionable clinical applicability and unknown biological relevance. The clinical and biological signature of PD may be unique to the individual, rendering PD resistant to meaningful cluster solutions. New approaches that acknowledge the individual-level heterogeneity and that are more aligned with personalized medicine are needed. (emphasis added).
Among the articles cited in the bibliography is this one (another open access article):
In this, the authors describe their methodology and results from the Oxford cohort (one of several cohorts of PwPs and controls that have been used for research. (I would take the time and effort to locate the original publication describing the different cohorts involved in the effort to find biomarkers, but I am currently experiencing a wave of Parkinson’s related apathy. Check my past posts, or do a search on PubMed – I do remember that Oxford and Boston were two of the cohorts of PwPs. But I digress).
Results: Apolipoprotein A1 and C-reactive protein levels differed across our PD subtypes, with severe motor disease phenotype, poor psychological well-being, and poor sleep subtype having reduced apolipoprotein A1 and higher C-reactive protein levels. Reduced apolipoprotein A1, higher C-reactive protein, and reduced vitamin D were associated with worse baseline activities of daily living (MDS-UPDRS II).
In other words: Close, but no cigar. But I, for one, certainly could have benefited from this knowledge had it been available 60 years ago. (don’t get me started – I’ve played that tape many times before).
Robert Cochrane is recruiting participants for a new Parkinson’s Disease study. See below. Note the three categories of PD people needed:
” We are recruiting male and female persons diagnosed with idiopathic (unknown cause) Parkinson’s disease between and fit ONE of the following criteria:
– They have been diagnosed within the last year,
– are early onset (diagnosed before the age of 50)
– are active or former members of the U.S. military. “”
Here’s the full recruitment flyer:
Participants needed for Narrative Study in Parkinson’s Disease Principal Investigator, Dr. Gabriele Wulf, and Robert Cochrane, PhD student at UNLV, are looking for persons with Parkinson’s disease to participate in an online research study of heroic narrative upon Parkinson’s disease. Study participants will be asked to share their perceptions and experiences about Parkinson’s from the time they were diagnosed to today, and how they feel about their future quality of life expectations. They will be taught heroic storytelling structure and practical tools of how to explore and incorporate it into their own lives. Heroic storytelling is based on the works of Joseph Campbell’s monomyth. Campbell’s work is broken into a 12-step journey for this class that participants will follow and use to write their own heroic journey with Parkinson’s disease. Participation in this study will require completion of 12 sessions, meeting once a week on Saturday mornings from 9a-10:30a (Pacific Time). Participants Will also be required to write a one-page personal assessment each week outside of class. Finally,online surveys at the beginning, middle and end of the 12-session period will be required. All sessions will take place online via Zoom. All sessions will be recorded. Participants must have a WiFi enabled device in a safe location (e.g. participants’ home) for these sessions. Sessions will include writing, theatrical improvisation and lectures from guest subject matter experts in fields such as dance, art and mythology. We are recruiting male and female persons diagnosed with idiopathic (unknown cause) Parkinson’s disease between and fit ONE of the following criteria:
– They have been diagnosed within the last year,
– are early onset (diagnosed before the age of 50)
– are active or former members of the U.S. military. Participants must be between 1-3 on the Hoehn and Yahr scale. This assessment should be given by participants’ neurologist or movement disorder specialist prior to acceptance into the program. We cannot accept persons who have an inability to communicate verbally, are uncomfortable writing, or are unable using the Zoom platform. Please email Robert Cochrane at cochra58@unlv.nevada.edu with questions or to express your interest in participating.This program was made possible, in part, by a grant from the Parkinson’s Foundation. Thank you!
The evidence that rhythm, movement, and making music continues to accumulate as a therapeutic approach to address the symptoms and Quality of Life issues related to Parkinson’s Disease (PD).
Today we look at an article just out in Frontiers of Human Neuroscience, titled
Over the last quarter of a century, increasing research results point to rhythm and music as effective and useful tools for treatment and rehabilitation of people with neurological disorders. This article reviews the evidence for four different approaches, what the consensus is at the present time, and, of course, suggests future directions.
The authors look at four different approaches:
Rhythmic Auditory Stimulation (RAS)
Music-Supported Therapy (MST)
Therapeutic Instrumental Music Performance therapy (TIMP) and
Patterned Sensory Enhancement (PSE)
The consensus of recent meta-analyses and systematic reviews is that, for Parkinson’s Disease (PD), is that RAS is an effective tool for improving gait, stride, and speed – folks walk faster and with longer steps with RAS. Additionally, evidence is showing that it also reduces freezing of gait (FOG), improves balance and reduces the occurrence of falls.
Neither MST nor TIMP have been studied much beyond the rehabilitation of stroke patients. They involve practicing on a keyboard or drums, beginning with the patient’s comfort level and increasing in difficulty. Some studies have begun to be used to investigate effectiveness as treatments for PD. Some have shown improvements in motor dexterity. More research is needed, but in the meantime, learning to play drums or keyboards can’t hurt, and may enrich one’s quality of life (QOL).
Growing evidence in neurological and brain imaging have shown increased activity in the auditory and motor areas of the brain, indicating that brain plasticity might be achieved through music and rhythmic interventions. The authors note that RAS has been well studied with stroke and PD populations, but not with other movement disorders and Alzheimer’s populations. In addition MST and TIMP have only begun to be investigated as a means of restoring fine motor coordination.
The authors also call for neuroimaging use in studies, to better understand the physiological basis of the rehabilitation process. They point out the gaps in research and hope to provide a framework for future research – not so much a roadmap, I would think, but a laying out of what we know and what we don’t know, and what kinds of studies are needed to answer the questions about what we don’t know.. They state that “musical rhythm is a powerful tool” for therapy, and our understanding and exploration of how it modulates brain networks is in the initial stages.
In other words, “We’ve only just begun.”
Meanwhile: Don’t stop moving to the music.
Citation: Braun Janzen T, Koshimori Y, Richard NM and Thaut MH (2022) Rhythm and Music-Based Interventions in Motor Rehabilitation: Current Evidence and Future Perspectives. Front. Hum. Neurosci. 15:789467. doi: 10.3389/fnhum.2021.78946
Diagnosis of PD is often not made until a person is in their 60s. With all the attention that has been focused on the disease(s) in the last 20 years or so, I suspect that more people are getting diagnosed at an earlier age, although most cases of young onset PD are likely to be genetic in origin.
However, an “early” diagnosis may not be a timely diagnosis, as the title of one opinion piece I read some time ago said (see link below).
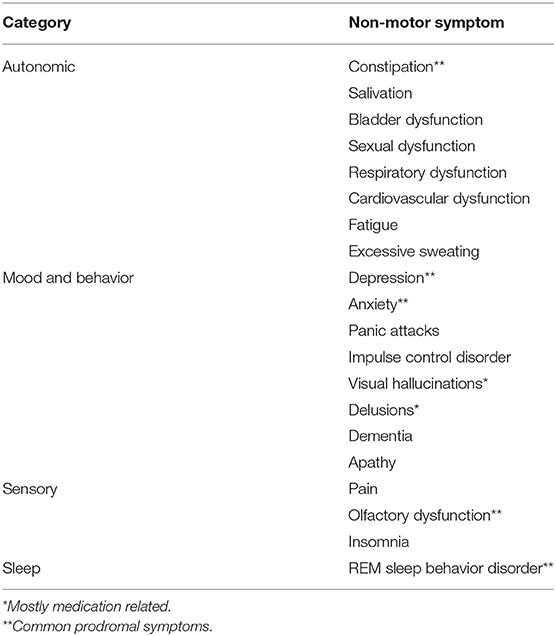
It is now becoming apparent that “Parkinson’s”includes several categories of symptoms, not just rigidity, tremors, and gait, as shown in the table below::
The problem is that treatment and diagnosis are often delayed until PD has already reduced Quality of Life for many folks.
Good evidence for the quality-of-life benefits of existing symptomatic treatment supports the argument for earlier diagnosis at a time when symptoms are already present (emphasis added). This argument would be significantly bolstered by the development of disease-modifying treatments. Benefits of early diagnosis and treatment would affect not only the individual (and their families) but also the wider society and the research community. Ultimately, however, shared decision-making and the principles of autonomy, beneficence, and non-maleficence will need to be applied on an individual basis when considering a “timely” diagnosis.
Therefore, the earlier one can predict the probability or inevitability of PD the sooner one can use treatments – whether pharmacological, surgical, nutritional, or lifestyle in nature – that can either reduce, delay, or defer (and possibly reverse?) the symptoms of PD.
Of all the symptoms associated with PD: tremors, bradykinesia, depression & anxiety, posture, gait issues (difficulties walking), REM Sleep Behavior Disorder (RBD), anosmia (loss of ability to smell), cognitive issues, facial masking, and micrographia (small handwriting) – RBD is the one which is most highly predictive of a later PD diagnosis.
The predictive ‘specificity’ is so strong that if someone has RBD, the chance of being diagnosed with Parkinson’s or related conditions over the next 15 years or more is over 80%
If an 18-21 year old person walked into a physician’s office with RBD, essential tremors, and depression as main symptoms, what would happen? In 1970, probably nothing – one might get treated for depression, but essential tremors are also called “benign”tremors, and were ignored, even if the patient reported being able to feel the tremors while resting, though invisible to the external observer. As for RBD, it would probably also be ignored.
By “a physician,” we are talking about a General Practitioner, or “family doctor,” and not s specialist like a Movement Disorders Specialist who would be trained to identify varied symptoms, including those that are prodromal. And, of course, the identification of prodromal symptoms has only been investigated within the last decade or so, and are identified as for “research only” purposes – not for clinical diagnosis. A recent survey article (not referenced below) indicated that a majority of general practitioners were either unaware of the Movement Disorders Society’s list of prodromal symptoms, or were not using them to make referrals to Movement Disorders Specialists.
But thanks to the dedication and generosity of folks like Michael J. Fox and others, PD has become a respectable disease for which the person who has it has no reason to be apologetic or ashamed, and can hold their head up (and they ought to, since one symptom is to walk with shoulders stooped down) and proudly proclaim that they have Parkinson’s, which is why they walk funny. And so it goes.
Articles that were quoted above or which contributed to this article are found in the links below.
This paper (or rather a chapter in a thesis) landed in my newsfeed recently. In it, the authors describe a study done to see whether people with Parkinson’s in the later stages are getting adequate treatment and whether they could benefit from more specific treatment. (A link to the PDf file is at the end of this post).
A person in Late Stage Parkinson’s has more than one of the following:
Motor symptoms not controlled despite medication.
Levadopa-related dyskinesias or dystonia,
PD dementia (defined according to MDS Task Force definition (Dubois et al. 2007), and not treated with cholinesterase inhibitors,
Depression not adequately treated,
Neuropsychiatric symptoms, such as agitation/ aggression; anxiety and irritability,
Orthostatic hypotension, pain, constipation, urinary symptoms, insomnia or daytime sleepiness (autonomic systems degeneration),
Falls on a regular basis,
Other symptoms related to risk of choking, speech issues, or producing too much saliva,
Inadequate Home environment.
Basically, the study provided a list of recommended activities and treatment on a sheet of paper (the control group) and actually providing the treatments and activities recommended, (the treatment group).
Not surprisingly, the treatment group did better at the end of the study than the controls. The conclusions were that people in late-stage Parkinson’s are often undertreated and could benefit from implementation of movement disorder specialists’ recommendations. (One would hope that the control group would also be provided with the treatments after the study ended. Perhaps, leading to another report)?
I’ve paraphrased the table used to describe late stage Parkinsonism in order not to infringe on their copyright. The title of the entire thesis is “Impairment and Disability in Late Stage Parkinsonism” and the overall author is Danny Hommel. I couldn’t find an email to ask for permission in writing to reproduce anything verbatim.
Other chapters include:
The late-stage of parkinsonism’s – motor and non-motor complications
The prevalence and determinants of neuropsychiatric symptoms in late-stage parkinsonism
Prevalence and prescribed treatments of orthostatic hypotension in institutionalized peoples with Parkinson’s disease (the chapter discussed in this post)
Optimizing treatment in undertreated late-stage parkinsonism: a pragmatic randomized trial
This isn’t in print yet, so I’ll just quote frm the abstract:
18 To date, no reliable clinically applicable biomarker has been established for Parkinson’s
19 disease (PD). Our results indicate that a long hoped blood test for Parkinson’s disease may
20 be realized. We here assess the potential of pathological α-synuclein originating from
21 neuron-derived exosomes from blood plasma as a possible biomarker. Following the
22 isolation of neuron-derived exosomes from plasma of PD patients and non-PD individuals
23 immunoblot analyses were performed to detect exosomal α-synuclein. Under native
24 conditions significantly increased signals of disease-associated α-synuclein forms in neuron25 derived exosomes were measured in all individuals with PD and clearly distinguished PD
26 samples from controls. By performing a protein misfolding cyclic amplification assay these
27 aggregates could be amplified and seeding could be demonstrated. Moreover, the
28 aggregates exhibited β-sheet-rich structures and showed a fibrillary appearance. Our study
29 demonstrates that the detection of pathological α-synuclein conformers from neuron-derived
30 exosomes from plasma samples has the potential of a promising blood-biomarker of PD.
Exosomes are small bundles of proteins enclosed by a membrane (if I understand it correctly)(feel free to correct me- the Wikipedia article hd a note saying that it was too technical for most readers – and I agree).
Exosomes contain material from the cells from which they originated, so might be used as biomarkers. Obviously, it will take a while to fund the research and develop some way to determine how far along the way to developing PD someone is. But the sooner a person can deal with it, the better the opportunity to live well with it. I look forward to the development of biomarkers that will help predict who might get Parkinson’s, so those folks can take preventive action.
I am fortunate that my symptoms did not appear in the usual sequence,and that I had DBS early after diagnosis, have had an outstanding medical team looking out for me and working with me, have a strong local community supporting people with Parkinson’s, and have a care partner who makes sure that my diet is full of organic foods, produce, and as few highly processed foods as possible. And I get lots of exercise, considering that I’m not athletic and I am not into weightlifting or bodybuilding.