We remember, fondly or not, typical school essay topics:
What I did last summer
How my family celebrates the winter holidays
What America means to me
My favorite (TV, movie, book, song, musical group)
Things my parents tell me not to tell other people
The greatest American President
I once wrote an essay about a relative. I actually took the question seriously, instead of offering the usual platitudes. I pondered on a negative experience: the untimely death of a child. This loss could have been prevented with more timely reliance on medical providers. Of course, this happened well before penicillin became widely available for treatment of appendicitis or peritonitis. As a parent, I promptly responded when my child complained of abdominal pain. She was treated for appendicitis and survived.
This past year, my summer was also related to a missed diagnosis. Fortunately, no one died, although I had been treated for the wrong condition for over a dozen years. It has been said that physicians bury their mistakes. Not this time. Instead, the differential diagnosis and removal of medications triggered research into the differentiation between Essential Tremors and Parkinson’s Disease. Another side effect was rewording this blog’s subtitle, replacing PD with Movement Disorder.
I submitted an abstract to the World Parkinson’s Conference. It will be held in May of 2026. Unfortunately, the abstract didn’t make the cut. Perhaps the abstract failed to include enough information, perhaps it didn’t have a positive enough bias in its presentation. Whatever. The research found misdiagnosis of movement disorders is not uncommon. Therefore I’ve decided to share it through this medium. Some people will find value in it.
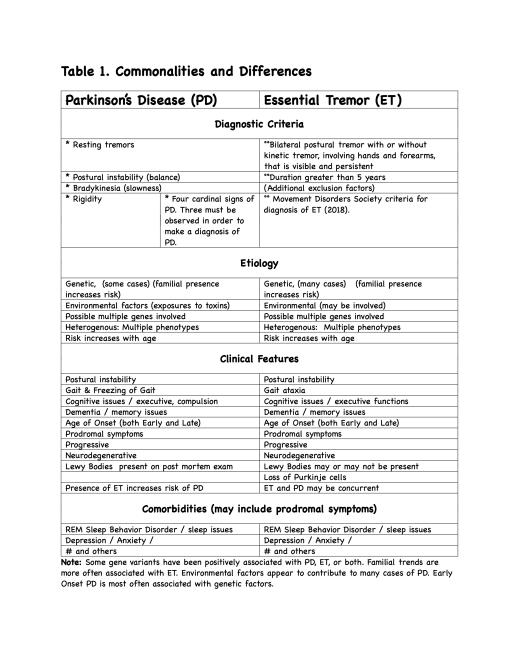
Below is a table from the article. In future posts, parts of the article will be shared, including the discussion, conclusions, and references by category.
Table 1. Commonalities and Differences (from an unpublished article on Misdiagnosis and Missed Diagnosis of Parkinson’s Disease and Essential Tremor
Non-Artificial Intelligence Summary: The author reveals that he was misdiagnosed with Parkinson’s Disease (PD) over 13 years ago, after initially seeking treatment for Essential Tremors (ET). The article concludes with a link to an open access article on Six Myths and Misconceptions about Essential Tremor.
_________________________
Over the summer of 2025, I’ve been undergoing review of my movement disorders, with a reduction in medications as well as no clinical observation of Parkinson’s Disease (PD) symptoms.
Some thirteen or so years ago, after a neurologist or nurse practitioner observed some slight rigidity, providing enough symptoms to make a clinical diagnosis, an old high school girlfriend called to express some concern and to wish me the best. Apparently, she was under the misconception that PD was equivalent to a slow death. Glad to say she must be mighty disappointed after all these years.
I had essential tremors (ET) from my teen years, in addition to several other prodromal conditions or symptoms relating to PD. In 2010 the ET had become somewhat disabling, and after many months of unsuccessful treatment for ET, I opted for Deep Brain Stimulation (DBS), which apparently had a great success rate with ET. However, in order to rule out PD, several months of tests were undergone, with the eventual three of four of the cardinal signs being observed. DBS was scheduled less than two months later. Seven years later, due to a lack of progressive neurological deterioration, a DAT Scan was ordered, with an interpretation that I apparently did have some form of parkinsonism. Apparently, the original diagnosis of PD was premature and made under the influence of confirmation bias. Or, to paraphrase Paul Simon, a person sees what they want to see and disregards the possibility of other underlying causes for a barely detectable symptom.
Finally, after moving to a different state and establishing care with a Movement Disorder Specialist, who conducted their own evaluation on and off PD medications, the original problem (ET) which brought me to a neurologist in 2010, was confirmed. The process of titrating off medications continues.
Naturally, I have been delving into the National Institutes of Health open access in order to learn more about what has been called “familial tremors” and “benign tremors” in the past.
One thing I have learned is the diagnosis of ET and PD can be difficult, due to many overlapping symptoms or conditions, they are linked genetically for some ET cases, and much of the material on PD doesn’t even investigate whether the two conditions are concurrent.
So another reason for me to go on living: educate and advocate for people who may or may not have a diagnosis appropriate to their condition.
And from the abstract and significance statement of the original (non-open access) article:
Physical exercise improves motor performance in individuals with Parkinson’s disease and elevates mood in those with depression. Although underlying factors have not been identified, clues arise from previous studies showing a link between cognitive benefits of exercise and increases in brain-derived neurotrophic factor (BDNF). (emphasis added).
and:
Exercise has been shown to improve movement and cognition in humans and rodents. Here, we report that voluntary exercise over 30 days leads to an increase in evoked dopamine (DA) release throughout the striatum, and an increase in BDNF in the dorsal (motor) striatum. The increase in DA release appears to require BDNF, indicated by the absence of DA release enhancement with running in BDNF+/- mice. Activation of BDNF receptors using a pharmacological agonist was also shown to boost DA release. Together these data support a necessary and sufficient role for BDNF in exercise-enhanced DA release, and provide mechanistic insight into the reported benefits of exercise in individuals with dopamine-linked neuropsychiatric disorders, including Parkinson’s disease and depression. (emphasis added).
The citation:
Voluntary exercise boosts striatal dopamine release: evidence for the necessary and sufficient role of BDNF, Guendalina Bastioli, Jennifer C. Arnold, Maria Mancini, Adam C. Mar, Begoña Gamallo-Lana, Khalil Saadipour, Moses V. Chao, Margaret E. Rice,Journal of Neuroscience 16 May 2022, JN-RM-2273-21; DOI: 10.1523/JNEUROSCI.2273-21.2022
So that covers why exercise is good for all. But what about what is good for the one?
… there is growing recognition that PD is not a single entity but instead reflects multiple diseases, in which different combinations of environmental, genetic and potential comorbid factors interact to direct individual disease trajectories… The clear consequence of there being distinct diseases that collectively form PD, is that there is no single biomarker or treatment for PD development or progression. We propose that diagnosis should shift away from the clinical definitions, towards biologically defined diseases that collectively form PD, to enable informative patient stratification. N-of-one type, clinical designs offer an unbiased, and agnostic approach to re-defining PD in terms of a group of many individual diseases. . (emphasis added).
The citation links to PubMed where you can download the full article, should you be so inclined. The next citation also links to an open access free article.
In this article, Riggare reports on self tracking done in 2012 (as a Person with Parkinson’s), and the offer the possibility that self-tracking of symptoms and medications can help to inform the physician’s decisions over the course of treatment. In other words, one should be a self-advocate as a patient and work with your physician to achieve the best combination of treatments to address Parkinson’s and its comorbidities. (At least that’s my takeaway from the article. Others might differ).
Another look at PD aims to categorize it into various sub-types:
This article is a “desk review”of other studies, using specific criteria to either include/exclude each study in the results. Their conclusion:
Conclusion: Subtyping studies undertaken to date have significant methodologic shortcomings and most have questionable clinical applicability and unknown biological relevance. The clinical and biological signature of PD may be unique to the individual, rendering PD resistant to meaningful cluster solutions. New approaches that acknowledge the individual-level heterogeneity and that are more aligned with personalized medicine are needed. (emphasis added).
Among the articles cited in the bibliography is this one (another open access article):
In this, the authors describe their methodology and results from the Oxford cohort (one of several cohorts of PwPs and controls that have been used for research. (I would take the time and effort to locate the original publication describing the different cohorts involved in the effort to find biomarkers, but I am currently experiencing a wave of Parkinson’s related apathy. Check my past posts, or do a search on PubMed – I do remember that Oxford and Boston were two of the cohorts of PwPs. But I digress).
Results: Apolipoprotein A1 and C-reactive protein levels differed across our PD subtypes, with severe motor disease phenotype, poor psychological well-being, and poor sleep subtype having reduced apolipoprotein A1 and higher C-reactive protein levels. Reduced apolipoprotein A1, higher C-reactive protein, and reduced vitamin D were associated with worse baseline activities of daily living (MDS-UPDRS II).
In other words: Close, but no cigar. But I, for one, certainly could have benefited from this knowledge had it been available 60 years ago. (don’t get me started – I’ve played that tape many times before).
Diagnosis of PD is often not made until a person is in their 60s. With all the attention that has been focused on the disease(s) in the last 20 years or so, I suspect that more people are getting diagnosed at an earlier age, although most cases of young onset PD are likely to be genetic in origin.
However, an “early” diagnosis may not be a timely diagnosis, as the title of one opinion piece I read some time ago said (see link below).
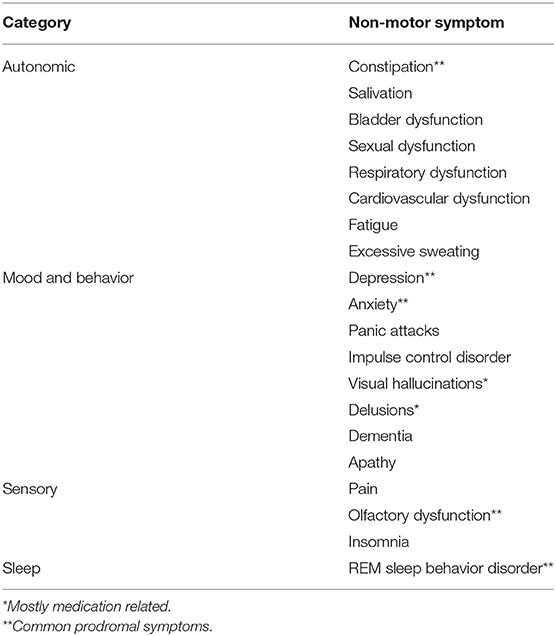
It is now becoming apparent that “Parkinson’s”includes several categories of symptoms, not just rigidity, tremors, and gait, as shown in the table below::
The problem is that treatment and diagnosis are often delayed until PD has already reduced Quality of Life for many folks.
Good evidence for the quality-of-life benefits of existing symptomatic treatment supports the argument for earlier diagnosis at a time when symptoms are already present (emphasis added). This argument would be significantly bolstered by the development of disease-modifying treatments. Benefits of early diagnosis and treatment would affect not only the individual (and their families) but also the wider society and the research community. Ultimately, however, shared decision-making and the principles of autonomy, beneficence, and non-maleficence will need to be applied on an individual basis when considering a “timely” diagnosis.
Therefore, the earlier one can predict the probability or inevitability of PD the sooner one can use treatments – whether pharmacological, surgical, nutritional, or lifestyle in nature – that can either reduce, delay, or defer (and possibly reverse?) the symptoms of PD.
Of all the symptoms associated with PD: tremors, bradykinesia, depression & anxiety, posture, gait issues (difficulties walking), REM Sleep Behavior Disorder (RBD), anosmia (loss of ability to smell), cognitive issues, facial masking, and micrographia (small handwriting) – RBD is the one which is most highly predictive of a later PD diagnosis.
The predictive ‘specificity’ is so strong that if someone has RBD, the chance of being diagnosed with Parkinson’s or related conditions over the next 15 years or more is over 80%
If an 18-21 year old person walked into a physician’s office with RBD, essential tremors, and depression as main symptoms, what would happen? In 1970, probably nothing – one might get treated for depression, but essential tremors are also called “benign”tremors, and were ignored, even if the patient reported being able to feel the tremors while resting, though invisible to the external observer. As for RBD, it would probably also be ignored.
By “a physician,” we are talking about a General Practitioner, or “family doctor,” and not s specialist like a Movement Disorders Specialist who would be trained to identify varied symptoms, including those that are prodromal. And, of course, the identification of prodromal symptoms has only been investigated within the last decade or so, and are identified as for “research only” purposes – not for clinical diagnosis. A recent survey article (not referenced below) indicated that a majority of general practitioners were either unaware of the Movement Disorders Society’s list of prodromal symptoms, or were not using them to make referrals to Movement Disorders Specialists.
But thanks to the dedication and generosity of folks like Michael J. Fox and others, PD has become a respectable disease for which the person who has it has no reason to be apologetic or ashamed, and can hold their head up (and they ought to, since one symptom is to walk with shoulders stooped down) and proudly proclaim that they have Parkinson’s, which is why they walk funny. And so it goes.
Articles that were quoted above or which contributed to this article are found in the links below.